


LARYNGEAL DISEASES
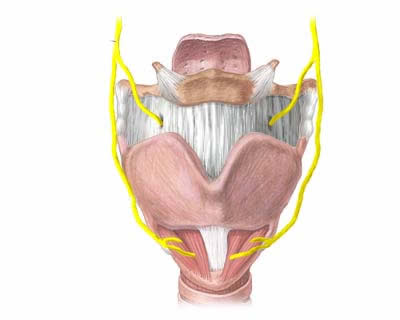 Larinx
Larinx The laryngeal diseases most commonly treated at our center include:
- acquired benign lesions of the vocal cords (nodules, polyps, cysts, granulomas, etc.).
- congenital benign lesions of the vocal cords (cysts, vergeture, sulcus Vocalis etc.).
- pre-cancerous laryngeal lesions (papillomatosis, dysplasia etc.)
- malignant laryngeal tumors
- functional dysphonias (non-organic / psychogenic)
- neurogenic dysphonias (paralysis, spasmodic dysphonia etc.)
- traumas
Introduced in 1972 by Strong and Jako for the treatment of a number of laryngeal conditions, the CO2 laser still remains the laser-based tool of choice in endoscopic laryngeal surgery due to its peculiar physical characteristics. The subsequent development of different energy emission techniques and that of micromanipulators capable of concentrating the incident beam to a diameter less than 300 microns (Acuspot and Acublade) have recently extended its field of use to include laryngeal microsurgery. The CO2 laser produces electromagnetic, non-ionizing energy falling in the field of infrared with a wavelength of 10.6 µ. Its unique physical characteristics warrant that the beam be handled through a complex system of mirrors and coupled with a helium-neon coaxial guidance laser. Its peculiar wavelength, which results in a high absorption coefficient in water and, as a consequence, a low rate of penetration through soft tissues, qualifies the CO2 laser as the optimal tool for minimizing thermal damage to tissues, the degree of which strictly depends on the amount and way in which the energy is released. Therefore, the surgical outcome will be a function of parameters such as power (in Watts), exposure time (milliseconds), spot diameter (microns), and way of emission (continuous, pulsed or superpulsed). The intraoperative advantages provided by the CO2 laser are due to the possibility of operating a single surgical instrument within the laryngoscope, improved surgical field control, as well as performing the procedure in the virtual absence of blood thanks to the laser’s efficacy in cutting tissue while at the same time cauterizing blood vessels less than 0.5 mm in diameter.
 Laryngostroboscopy in normal subject
Laryngostroboscopy in normal subject  Laringostroboscopia carcinoma corda
vocale destra
Laringostroboscopia carcinoma corda
vocale destra